Table of Contents

Multimorbidity in India: Why Chronic Care Needs Urgent Reform
India is no longer battling only infectious diseases. A muted, more complex crisis is unfolding, one where millions are living not with a single illness, but with several chronic conditions at the same time.
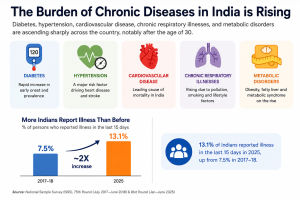
Diabetes, hypertension, cardiovascular disease, chronic respiratory illnesses, and metabolic disorders are ascending sharply across the country, notably after the age of 30. Recent National Sample Survey (NSS) data reveal that 13.1% of Indians reported illness during a 15-day period in 2025, approximately double the 7.5% recorded in 2017- 18. Among adults above 60 years, the figure rises perilously to 43.9%.
This is the reality of multimorbidity, the concurrence of two or more chronic conditions in one individual. And as India’s population ages, multimorbidity is rapidly becoming one of the country’s most pressing public health and health policy challenges.
Why chronic care is fragmented
India’s healthcare system still tends to treat diseases separately, even when patients experience them together. A person with diabetes may visit one doctor, consult another for hypertension, undergo tests at multiple facilities, and receive prescriptions from several providers, often without coordination between them. The result is fragmented care, repeated diagnostics, overlapping medicines, and growing confusion for patients and caregivers alike.
This fragmentation fuels another major concern: polypharmacy, or the simultaneous use of multiple medications. For elderly patients, taking five, six, or even nine medicines a day is no longer unusual. Without integrated treatment plans or interoperable health records, harmful drug interactions and avoidable Adverse Drug Reactions (ADRs) become increasingly common. The consequences are costly, both medically and financially.
The financial burden
India already faces high out-of-pocket expenditure (OOPE), with average hospitalization costs exceeding ₹34,000. For many families, the burden extends far beyond hospitalization. Chronic illnesses demand continuous spending on medicines, diagnostics, consultations, and long-term follow-up care. For uninsured households, this often pushes healthcare costs into financial catastrophe.
The answer cannot lie in treating one disease at a time.
India now needs a shift towards integrated, patient-centred care, a model that organizes healthcare around the individual rather than isolated illnesses. Strengthened Primary Health Centres (PHCs) and Ayushman Arogya Mandir (AAMs) must become long-term care coordinators, managing referrals, medication reviews, and continuity of care across providers.
The role of digital health
Digital health infrastructure will play a defining role in this transition. The Ayushman Bharat Digital Mission (ABDM), supported by ABHA (Ayushman Bharat Health Account) IDs, can enable interoperable electronic health records that reduce duplication, improve medication safety, and ensure continuity across the care pathway.
But integrated care is not only about technology. It is also about restoring the patient’s voice. Too often, individuals navigating multiple illnesses feel overwhelmed, unheard, and disconnected from decisions shaping their treatment. Sustainable healthcare systems must empower patients, caregivers, and families as active participants in care.
India’s health transition demands more than expanded coverage. It demands coordinated systems, connected data, stronger primary healthcare, and care models built around people, not diseases.
Without that shift, multimorbidity and polypharmacy may become the country’s next silent public health emergency.
To see how India can strengthen health systems for people living with chronic and multiple conditions, you can explore ISPP’s Centre for Universal Health Assurance.